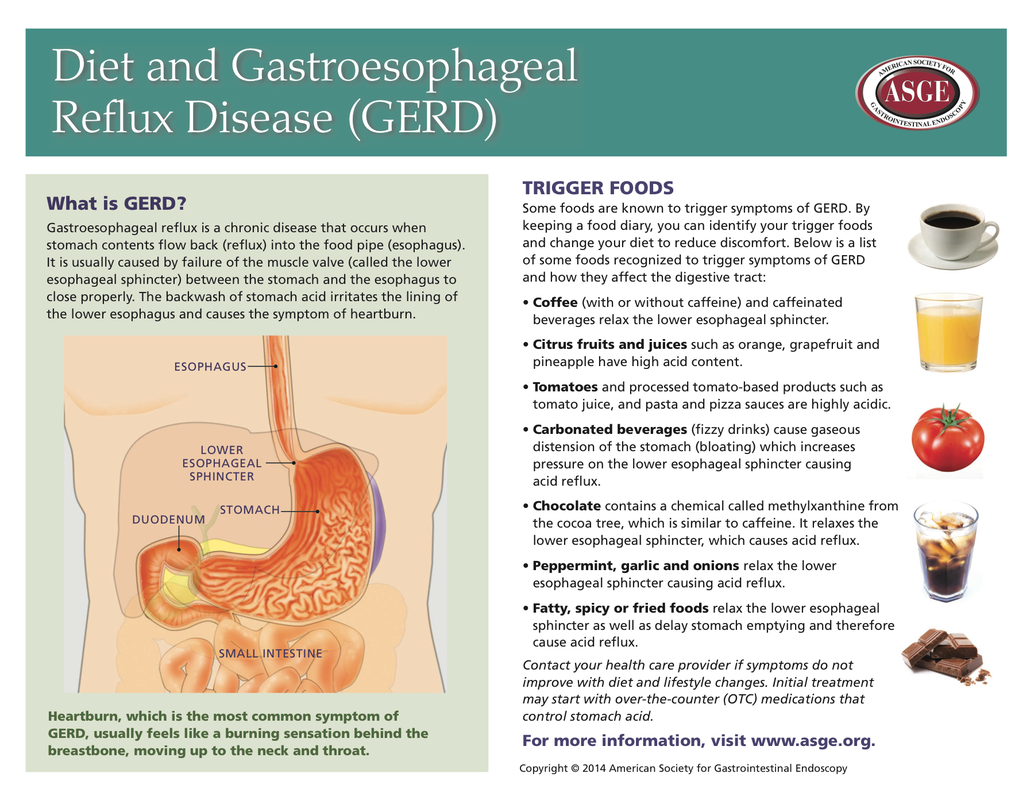
Definition of Gastroesophageal reflux (GERD) :
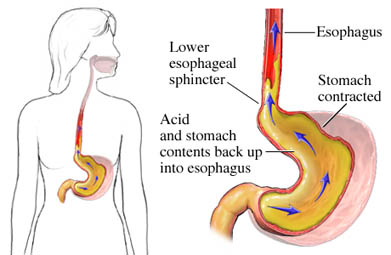
Severe “heartburn” in laymen’s language. Weakness of the valve between the oesophagus and stomach may allow stomach acid to reflux (regurgitate, backup) into the oesophagus and irritate and inflame the lining. This results in chest pain which can mimic that of angina (pain of cardiac ischemia or an MI).
Severe “heartburn” in laymen’s language. Weakness of the valve between the oesophagus and stomach may allow stomach acid to reflux (regurgitate, backup) into the oesophagus and irritate and inflame the lining. This results in chest pain which can mimic that of angina (pain of cardiac ischemia or an MI).
Signs and symptoms
- A burning sensation in your chest (heartburn), sometimes spreading to your throat, along with a sour taste in your mouth
- Chest pain
- Difficulty swallowing (dysphagia)
- Dry cough
- Hoarseness or sore throat
- Regurgitation of food or sour liquid (acid reflux)
- Sensation of a lump in your throat
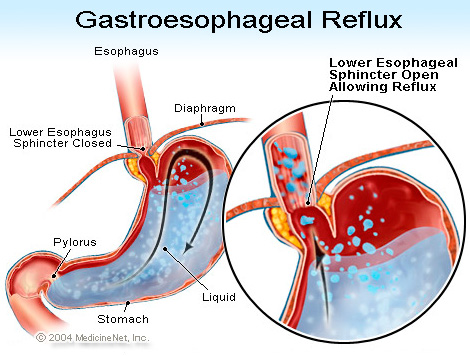
Causes of gastroesophageal reflux disease
GERD is caused by a failure of the lower oesophageal sphincter. In healthy patients, the "Angle of His"—the angle at which the oesophagus enters the stomach—creates a valve that prevents duodenal bile, enzymes, and stomach acid from travelling back into the oesophagus where they can cause burning and inflammation of sensitive oesophageal tissue.
Factors that can contribute to GERD:
- Hiatal hernia, which increases the likelihood of GERD due to mechanical and motility factors.
- Obesity: increasing body mass index is associated with more severe GERD. In a large series of 2,000 patients with symptomatic reflux disease, it has been shown that 13% of changes in oesophageal acid exposure is attributable to changes in body mass index.
- Zollinger-Ellison syndrome, which can be present with increased gastric acidity due to gastrin production.
- A high blood calcium level, which can increase gastrin production, leading to increased acidity.
- Scleroderma and systemic sclerosis, which can feature oesophageal dysmotility.
- The use of medicines such as prednisolone.
- Visceroptosis or Glénard syndrome, in which the stomach has sunk in the abdomen upsetting the motility and acid secretion of the stomach.
|
|
GERD has been linked to a variety of respiratory and laryngeal complaints such as laryngitis, chronic cough, pulmonary fibrosis, earache, and asthma, even when not clinically apparent. These atypical manifestations of GERD are commonly referred to as laryngopharyngeal reflux (LPR) or as extraesophageal reflux disease (EERD).
Factors that have been linked with GERD, but not conclusively:
Factors that have been linked with GERD, but not conclusively:
- Obstructive sleep apnea
- Gallstones, which can impede the flow of bile into the duodenum, which can affect the ability to neutralize gastric acid
Diagnosis
Diagnosis and Diagnostic Testing of the Esophagus/Stomach
A detailed history is vital for an accurate diagnosis. Useful investigations may include ambulatory Esophageal pH Monitoring, barium swallow X-rays, esophageal manometry, and Esophagogastroduodenoscopy (EGD).
Esophagogastroduodenoscopy (EGD)
It involves insertion of a thin scope through the mouth and throat into the esophagus and stomach (usually while the patient is sedated) in order to assess the internal surfaces of the esophagus, stomach, and duodenum. Biopsies (taking samples of the tissure) can also be performed during endoscopy. This is probably the single most important test that anyone with GERD should have. It is the only way to detect damage and complications early when they are easier to treat. Many of the complications of GERD have no symptoms until they are very advanced and difficult to treat.
Esophageal pH Monitoring.
It is the current gold standard for diagnosis of gastroesophageal reflux disease (GERD). It provides direct physiologic measurement of acid in the esophagus and is the most objective method to document reflux disease, assess the severity of the disease and monitor the response of the disease to medical or surgical treatment. It can also be used in diagnosing laryngopharyngeal reflux.
In the past, an indwelling nasoesophageal catheter was the only way to measure esophageal acid exposure. Because this method is associated with nasal and pharyngeal discomfort and rhinorrhea, patients may have limited their activity and become more sedentary during the monitored period. This may have resulted in less reflux and a false negative test. The Bravo pH monitor is a catheter-free radio telemetric system which allows a longer period of monitoring and is better tolerated.
A detailed history is vital for an accurate diagnosis. Useful investigations may include ambulatory Esophageal pH Monitoring, barium swallow X-rays, esophageal manometry, and Esophagogastroduodenoscopy (EGD).
Esophagogastroduodenoscopy (EGD)
It involves insertion of a thin scope through the mouth and throat into the esophagus and stomach (usually while the patient is sedated) in order to assess the internal surfaces of the esophagus, stomach, and duodenum. Biopsies (taking samples of the tissure) can also be performed during endoscopy. This is probably the single most important test that anyone with GERD should have. It is the only way to detect damage and complications early when they are easier to treat. Many of the complications of GERD have no symptoms until they are very advanced and difficult to treat.
Esophageal pH Monitoring.
It is the current gold standard for diagnosis of gastroesophageal reflux disease (GERD). It provides direct physiologic measurement of acid in the esophagus and is the most objective method to document reflux disease, assess the severity of the disease and monitor the response of the disease to medical or surgical treatment. It can also be used in diagnosing laryngopharyngeal reflux.
In the past, an indwelling nasoesophageal catheter was the only way to measure esophageal acid exposure. Because this method is associated with nasal and pharyngeal discomfort and rhinorrhea, patients may have limited their activity and become more sedentary during the monitored period. This may have resulted in less reflux and a false negative test. The Bravo pH monitor is a catheter-free radio telemetric system which allows a longer period of monitoring and is better tolerated.
Treatment - pharmacology/non-pharmacology
Three types of treatments exist for GERD. These include lifestyle modifications, medications, and surgery. In patients with severe symptoms life-style modifications have showed limited benefit.
Medications
A number of drugs are approved to treat GERD, and are among the most prescribed medication in Western countries.
Surgical Treatment
A Biomechanical Malfunction
As complex as the reflux issue appears, the solution is relatively straightforward because reflux and its complications are actually caused by a biomechanical malfunction-a loose valve (LES) at the end of the esophagus. The pharynx, esophagus and stomach are basically mechanical organs. They don't absorb food or nutrients but rather are designed to function in the process of ingestion -taking in the food and preparing it for the small intestine, where absorption becomes the important function. Thus, the solution to the problem of reflux is to correct the mechanical problem (the loose valve) through surgery. Antireflux procedures such as Nissen fundoplication re-establish the barrier (valve) between the esophagus and stomach, and keep both gastric and duodenal juice out of the esophagus, abolishing the environment that places patients at risk for Barrett's metaplasia.
Minimally Invasive Surgical Approaches to Treat Reflux Disease
The Laparoscopic Nissen Fundoplication procedure is used to construct a new valve between the stomach and the esophagus. The stomach is pulled up and around the esophagus, then secured around the esophagus, and the valve is then placed into the abdomen below the diaphragm. In the past, an open surgical procedure was necessary to surgically stop gastroesophageal reflux in patients with severe disease. Today this can be done laparoscopically. Small ports are pushed through the belly wall (4 to 5 are used). One contains a video camera and shows the surgeon the inside of the abdomen. This allows the defective valve between the esophagus and stomach to be augmented without opening the abdomen. Much of the work in laparoscopic Nissen fundoplication was pioneered at USC. Designed to reconstruct the valve between the stomach and esophagus to eliminate gastroesophageal reflux, the surgery entails a complete 360-degree fundoplication where the upper stomach is folded around the lower esophagus. The procedure takes approximately 1-2 hours and patients can return home one or two days after the operation.
While some patients with severe reflux disease may benefit from the laparoscopic Nissen fundoplication, which is a 360 Degree valve, others with esophageal motility disorder may benefit from a partial valve, a 270 Degree
Laparoscopic Toupet Fundoplication.
For short esophageal length, a Collis gastroplasty (using part of the stomach to add length to the esophagus) and constructing a fundoplication over the added "neo-esophageal" segment represents the optimal approach.
Medications
A number of drugs are approved to treat GERD, and are among the most prescribed medication in Western countries.
- Proton pump inhibitors (such as omeprazole, esomeprazole, pantoprazole, lansoprazole, and rabeprazole) are the most effective in reducing gastric acid secretion. These drugs stop acid secretion at the source of acid production, i.e., the proton pump. The long term use of these medications may have adverse side effects.
- H2 receptor blockers (such as ranitidine, famotidine and cimetidine) can reduce gastric secretion of acid. These drugs are technically antihistamines. They relieve complaints in about 50% of all GERD patients.
- Sucralfate (Carafate) is also useful as an adjunct in helping to heal and prevent esophageal damage caused by GERD, however it must be taken several times daily and at least two (2) hours apart from meals and medications.
- Baclofen is an agonist of GABAB receptor. In addition to its skeletal muscle relaxant properties, it has also been shown to decrease transient lower esophageal sphincter relaxations at a dose of 10mg given four times daily.
Surgical Treatment
A Biomechanical Malfunction
As complex as the reflux issue appears, the solution is relatively straightforward because reflux and its complications are actually caused by a biomechanical malfunction-a loose valve (LES) at the end of the esophagus. The pharynx, esophagus and stomach are basically mechanical organs. They don't absorb food or nutrients but rather are designed to function in the process of ingestion -taking in the food and preparing it for the small intestine, where absorption becomes the important function. Thus, the solution to the problem of reflux is to correct the mechanical problem (the loose valve) through surgery. Antireflux procedures such as Nissen fundoplication re-establish the barrier (valve) between the esophagus and stomach, and keep both gastric and duodenal juice out of the esophagus, abolishing the environment that places patients at risk for Barrett's metaplasia.
Minimally Invasive Surgical Approaches to Treat Reflux Disease
The Laparoscopic Nissen Fundoplication procedure is used to construct a new valve between the stomach and the esophagus. The stomach is pulled up and around the esophagus, then secured around the esophagus, and the valve is then placed into the abdomen below the diaphragm. In the past, an open surgical procedure was necessary to surgically stop gastroesophageal reflux in patients with severe disease. Today this can be done laparoscopically. Small ports are pushed through the belly wall (4 to 5 are used). One contains a video camera and shows the surgeon the inside of the abdomen. This allows the defective valve between the esophagus and stomach to be augmented without opening the abdomen. Much of the work in laparoscopic Nissen fundoplication was pioneered at USC. Designed to reconstruct the valve between the stomach and esophagus to eliminate gastroesophageal reflux, the surgery entails a complete 360-degree fundoplication where the upper stomach is folded around the lower esophagus. The procedure takes approximately 1-2 hours and patients can return home one or two days after the operation.
While some patients with severe reflux disease may benefit from the laparoscopic Nissen fundoplication, which is a 360 Degree valve, others with esophageal motility disorder may benefit from a partial valve, a 270 Degree
Laparoscopic Toupet Fundoplication.
For short esophageal length, a Collis gastroplasty (using part of the stomach to add length to the esophagus) and constructing a fundoplication over the added "neo-esophageal" segment represents the optimal approach.
Statistics
Prevalence and Occurrence
- Sixty percent of the adult population will experience some type of gastroesophageal reflux disease (GERD) within a 12 month period and 20 to 30 percent will have weekly symptoms. 1
- Approximately seven million people in the United States have some symptoms of GERD. 2
- In 2004, approximately 20 percent of the United States population reported reflux symptoms that occurred at least weekly. 3
- Yearly hospitalizations with obesity diagnoses increased in the United States by 112 percent between 1996 and 2004. Obesity is linked to the development of GERD and frequency of symptoms. 1
- Primary or secondary GERD diagnosis increased by an unprecedented 216 percent or from a total of 995,402 individuals diagnosed in 1998 to 3,141,965 in 2005. 1
- Children with GERD symptoms who were hospitalized with a primary GERD diagnosis increased by 42 percent in infants and 84 percent in children between the ages of two and 17. 1
- In 2005, 9.1 percent of hospitalizations for GERD also included health concerns such as weight loss, vomiting, and anemia. These symptoms can signal GERD and other esophageal disorders. 1
- 4.2 percent of all people hospitalized with GERD in 2005 also had an esophageal disorder. From 1998 to 2005, other esophageal disorders also had a higher rate of diagnosis of GERD with dysphagia (264 percent), esophageal adenocarcinoma (195 percent) and esophagitis (94 percent). 1
- In the United States, 1,150 deaths in 2004 were directly related to a primary diagnosis of GERD. 3
- Individuals that report weekly reflux symptoms have been affected by the symptoms for more than five years. 4
- In a 2000 mail survey, 130, 000 individuals reported that they had signs of reflux disease and heartburn. Of these, 95 percent reported symptoms occurring for more than one year and half reported symptoms that had occurred for more than five years. Of these, 75 percent reported that the symptoms occurred at least twice a week. 4
- Fifty percent of all people questioned regarding GERD symptoms report that they have more heartburn at night than in the day. Sixty-three percent reported difficulty sleeping and 40 percent reported that daily functioning was compromised the next day. 4
- Approximately one percent of all people in the United States with a diagnosis of GERD also have a condition known as Barrett's esophagus. This is more commonly seen in men, particularly Caucasian men, and rarely occurs in children. There are no specific symptoms associated with Barrett's esophagus, and usually the diagnosis of GERD also finds the changes in the esophagus that are consistent with this condition. The average age of diagnosis for Barrett's esophagus is 50, which is consistent with the timing of the diagnosis of GERD for many adults.
- In 2004, there were 18.3 million ambulatory care visits to healthcare professionals in emergency rooms, physicians’ offices, and clinics. 3
- Approximately 3.1 million people were hospitalized in the United States in 2004 for GERD-related symptoms, complications, and treatment. 3
- There are approximately 64.6 million prescriptions written for GERD medications in the United States on an annual basis. 3
- Approximately 5 percent of all patient consults that a primary care physician completes will be related to GERD. 4
- People with GERD have a lower reported health-related qualify of life, which includes reduced enjoyment of food (80 percent), sleep problems (60 percent), and work concentration difficulties when symptoms were present (40 percent). 4
- It’s estimated by the American College of Gastroenterology that the symptoms of GERD result in almost $2 billion in lost productivity each week of the year. 5
|
|
|
|
|
|
